A High School Q&A About Covid–19

Students and teachers have as many questions about Covid-19 as anyone. Here we answer questions posed by Ms. Tara Stremic, a biology teacher at Broughton High School in Raleigh, North Carolina and her students. These are a mix of questions aimed at making sense of how Covid-19 impacts our (and their) daily lives and questions that help to fit the unfolding evolutionary story of the virus that causes Covid-19 into the unfolding (and now online) high school biology curriculum. Below, Dr. Matt Koci, a virologist at North Carolina State University answers Tara’s questions.
 Ms. Stremic: How exactly did the SARS-CoV-2 virus jump from an animal host to humans in Wuhan (was it eaten, breathed in?)
Ms. Stremic: How exactly did the SARS-CoV-2 virus jump from an animal host to humans in Wuhan (was it eaten, breathed in?)
 Dr. Matt Koci: The short and honest answer is we don’t know for sure, but there is no evidence that the virus is being transmitted in food. All evidence is this is primarily being spread like the flu or other cold viruses, in coughs and sneezes. So I would assume the first jump was also by breathing it in. That assumption is based on what we think happened in the early 2000s with the first SARS-Coronavirus. Food handlers in live animal markets, who had more direct contact with the live animals were at higher risk of getting the disease than others, suggesting that eating infected food wasn’t a major means of transmission.
Dr. Matt Koci: The short and honest answer is we don’t know for sure, but there is no evidence that the virus is being transmitted in food. All evidence is this is primarily being spread like the flu or other cold viruses, in coughs and sneezes. So I would assume the first jump was also by breathing it in. That assumption is based on what we think happened in the early 2000s with the first SARS-Coronavirus. Food handlers in live animal markets, who had more direct contact with the live animals were at higher risk of getting the disease than others, suggesting that eating infected food wasn’t a major means of transmission.
Ms. Stremic: What determines how a virus is transmitted from host to host? Is it just the outer viral proteins?
Dr. Matt Koci: I’m assuming you’re asking within a species, which is to say, “what determines how it moves from person-to-person?”
So in the case of coronavirus, what determines it would be spread by coughs and sneezes and not by mosquitos, right? Thinking of host-to-host in this case, the answer is typically a function of where in the body does it replicate and what’s the least complicated way it can get to that same tissue in a new host. So if you’re a virus that replicates in the lung, the easiest path to a new lung is to be coughed out and breathed into someone else. If you’re a virus-like norovirus that replicates in the intestine and causes diarrhea, your shortest distance to a new host is causing your host to poop all over the place in the hopes that someone swallows some of the resulting mess (life is gross) and you find your way into the intestine of someone new.
Now if by host-to-host you mean from one species to another, that’s a little different. Here yes, the outer proteins play a big part, but that’s just one step in the chain. The host cell receptor in the new host (species) needs to be similar enough to the cell receptor in the original species that the virus can bind to it, even if the binding isn’t perfect. If that condition is met, all the other steps associated with virus entry into the cell also need to be similar enough. If the virus requires other host proteins (secondary receptors or host enzymes) they also have to be present at the right concentration and conserved between host species so the virus can recognize and use those, too. Then, once the virus gets inside and uncoats and starts to replicate (see answer below about life cycle) all the other viral proteins used to take over the cell, they need to recognize these other host proteins, especially those whose job is focused on blocking innate immune defenses.
Ms Stremic: Does the shape/size/genome size of a virus correlate to its fatality/contagiousness?
Dr. Matt Koci: No. There are viruses of all different types, shapes, and sizes (physically and genomically). What makes one more contagious or deadly than another has to do with the proteins it makes and how those proteins interact with your cells. A good example of that is the common cold coronaviruses; these aren’t deadly, but they are the same size and shape as SARS-Cov-2. There are viruses that are much smaller than coronavirus that are much deadlier (Ebola comes to mind) and there are others that are even bigger that can be worse, think smallpox (we eradicated that decades ago). In each family of viruses, there can be a lot of variability in how they behave and the diseases they cause (we talk about how SARS-Cov-2 compares in size to other common viruses on this blog).
Ms Stremic: What are the types of cells in the body that this particular virus affects and what steps does it go through to make more copies of itself?
Dr. Matt Koci: So this virus uses the host cellular receptor ACE2 (angiotensin-converting enzyme 2). ACE2 is expressed on a lot of cells, so it has the ability to bind to, and possibly infect lots of different cells of the body. It is still not clear how many different cells the coronavirus is replicating in. Clearly, cells of the respiratory tract are involved, but there is also some evidence that maybe intestinal cells are also infected, but it could be others. It’s also not clear if the replication in these other cells is tied to worse disease.
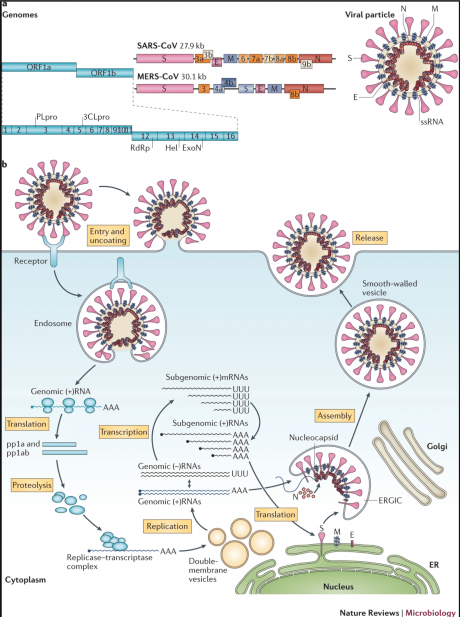
The way this virus typically works (and several other enveloped viruses) is when the virus binds it triggers the cell to pull it inside (internalization) through a process known as endocytosis. This gets the virus inside the cell, but it’s not really inside the cell yet. It’s trapped inside a vesicle. To start taking over the cell and replicating, it needs to get out of the vesicle and release its genes and proteins into the cytoplasm. To do this, the Spike protein needs to be cut into 2 parts. This is called enzymatic cleavage and is typically done by host enzymes. This allows for the spike protein to change shape in a way that allows for the lipids in the virus coat and vesicle to fuse. This membrane-membrane fusion event triggers what’s called “uncoating”. So this fusion event is critical, which means the ability of the viral receptor protein to be cut is a critical step in the virus life cycle and regulating what cells/tissues it can infect (tissue tropism). Several host enzymes have been suggested to play a role in this cleavage step; furin, cathepsin L and TMPRSS2, all trypsin-like proteases. I should also note that there is some evidence that the membrane fusion step can occur without endocytosis, so that step may not be necessary, but the cleavage of the spike to allow for membrane fusion is still a key step.
After uncoating, the viral RNAs are released into the cytoplasm of the cell. In the case of coronavirus, the RNA genome is what’s called positive-sense RNA. That means the viral RNA looks like messenger RNA to the host cell and starts making proteins off the viral genome, and this is really the start of the infection. (As a side note, the genomes of other RNA viruses like influenza are negative-sense RNA viruses. Their RNA genome is the reverse complement of messenger RNA, so the cell doesn’t make protein off it right away. These viruses bring along their own polymerase capable of making new RNA strands of RNA templates. When these viruses first uncoat, the viral polymerase converts the negative since RNA genome into positive-sense RNA that the cell then sees as mRNA and the infection takes off).
Once the cell starts making the viral proteins they (viral proteins) start doing their specific jobs. Some proteins are focused on “hijacking” the cell, making sure the cell’s machinery is dedicated to making virus products and not host products that the virus doesn’t need. Other proteins are involved in blocking host cell defenses against viruses. While other proteins are dedicated to making as many copies of new daughter genomes as possible. Once the cell has been largely exhausted of resources, the process reverses itself. The virus stops making copies of itself and starts to assemble new viral particles. In coronaviruses, a protein known as N binds to the RNA genome to help protect it, and shuttle the RNA to the place in the cell where it will be packaged into a new virus. For enveloped viruses, the structural membrane proteins (S, M, and E) will be inserted in a host membrane, the RNA will then bud through that membrane so the “vesicle” that comes off is a newly packaged virus with RNA inside. This is then released from the cell to go off and infect new cells.
To look at this process another way check out this video. It is from a biotech company trying to sell their technology for how to treat/prevent flu infections, but a lot of the principles are the same for coronavirus. Just don’t worry with anything after 2min 25s:
Ms Stremic: What specific immune system cells are involved that respond to this virus?
Dr. Matt Koci: In short, all of them. What we don’t know is which ones are helpful. It’s thought that in some of the most severe cases, a lot of the lung damage is from an overly aggressive immune response, but what cells drive that response and which cells lead to less severe disease is not clear. It does appear that antibodies are protective, so B-cell responses are clearly involved and likely a good thing. Being a viral infection killer T-cells are going to play a role, as are helper T-cells in coordinating the response of the others, but the devil is in the details on this response and right now we just don’t know enough details.
Ms Stremic: Why are different people more immune to the virus than others? What makes some people asymptomatic?
Dr. Matt Koci: This is the billion-dollar question right now, and we don’t know why some people are asymptomatic and others require serious medical help. We don’t even know how many people are asymptomatic. Hopefully, we will start testing more people, not just for the virus, but to see if they have antibodies to the virus to show that they were infected but didn’t get sick. Once we identify enough of these people we’ll be able to start to figure out what’s different between these groups.
This is a subtle difference, but I don’t think the asymptomatic people are immune. As far as we know today, this virus is so new and so different, no one should have prior immunity. We’ll likely find that some people are genetically resistant like we found with HIV and other diseases. We know the primary receptor for HIV is CD4 on CD4 positive T-cells; however, HIV also needs another protein, CCR5. We actually figured that out when we identified some people who seemed to be resistant to infection and found that they had mutations in their CCR5 gene, so it wasn’t expressed. There may be something like that involved here. Another explanation is the severity of the disease is related to how aggressively your immune system reacts to the infection. Because of other medical conditions, other lung infections you’ve had, or other factors we don’t understand, in some people the immune system overreacts and ends up causing more damage than the virus does. This was also true with the first SARS outbreak, as well as people who have contracted the H5N1 bird flu. However, what causes the overreaction in some and not others is largely unknown.
One last comment on this, if you’re interested in how different infectious diseases have shaped human evolution and how some of the genetic diseases of today may be the results of disease selection pressure in the past, this–Survival Of The Sickest–is a good book.
Ms. Stremic: How long have viruses been around and what is the first ever documented case of a virus infecting humans?
Dr. Matt Koci: Viruses have been around likely since there have been cells. In fact, there’s one theory that self-replicating RNA (not that different from an RNA virus) might actually have developed before cell-based life. We’ll never know for sure, but without a doubt, viruses were around before humans, and so as soon as humans arrived, there would have been viruses to infect them. There is a small but growing field of viral archeology where people look for evidence that viruses played a role in some of the major events in early human history. For example, several viruses have been implicated as being part of the 10 plagues in the book of Exodus in the Bible.
Ms. Stremic: If viruses are not living, how does hand washing “kill” viruses?
Dr. Matt Koci: I love this question. So virologists and biologists continually debate what is the meaning of life. You would think defining what life is would be easy but it turns out it’s like defining what smart is. The definition that I think most people still learn is something like; it has the capacity to grow, metabolize, respond (to stimuli), adapt, and reproduce. Based on this definition viruses aren’t alive only because grow, metabolize, and respond don’t fit, but everything else fits. They don’t grow because they never change size. They assemble. You will hear people say the virus grows in the lung, or something like that, but what they really mean is it replicates there. And the viruses require a lot of energy, nucleic acids, proteins and lipids, but they can’t make any of that on their own so they can’t metabolize. And they don’t run away if you poke them with a stick, but they do evolve in response to stimuli so it depends on how you define “respond”. I should say there are other definitions for life that some people use that have fewer criteria and under that definition viruses might qualify as a form of life.
Given how much they can do with so few genes, I certainly think they should be considered alive–why else would you learn about them in biology class? However, the general consensus among scientists is that they technically aren’t alive, so I’ll get off my soapbox and get back to your question. You’ll hear people talk about “killing” viruses, but when virologist talk we refer to it as “inactivating” the virus. In virology, viruses are either active (or they could also be referred to as infectious) OR they inactive. But, these distinctions typically aren’t that critical, so when non-virologist say things like “live virus vaccine”, “handwashing kills viruses”, or even the “virus grows in the lung” most virologists don’t get worked up about it. We recognize that words like active, inactive, replicate, and propagate are science jargon and might cause more confusion for others, so as long as the underlying concept being communicated is correct, that’s the important part. In fact, most of us use these phrases ourselves from time to time, but if you do and another virologist hears you, you’ll get a sarcastic, “Are you saying viruses are alive?”
So one other point to make about handwashing. You hear a lot in the news about handwashing vs. using hand sanitizer, and which is better at “killing” the virus. In both cases it’s about contact time. You need enough sanitizer to completely cover your hands, and the alcohol in the sanitizer needs to not evaporate off too quickly. Any virus that isn’t “killed” by the sanitizer is still on your hands. When you use soap and water, it’s also about contact time, that’s why they tell you to scrub for at least 20 seconds. The soap works on the lipids in the virus, but the water helps flush stuff off your hands, and then when you follow up by drying your hands with a paper towel you’re hopefully removing any more left behind. That said, either method is magic. They have to be done properly, and the more you do it the safer you’ll be. For good tips see the CDC’s page on handwashing.
Ms. Stremic: If we’re developing a vaccine for Covid-19, why don’t we have a vaccine for the common cold?
Dr. Matt Koci: This is another good question. I’m not sure the exact reason for this, but I suspect it related to 2 factors. First, while there are several coronaviruses that commonly cause the common cold, there are roughly 200 viruses from all different types of virus families (not coronaviruses) that can cause the common cold (the cold is really a set of multiple diseases with similar systems). To make vaccines to all these would just be too expensive to prevent a disease that while unpleasant for a few days, isn’t really life-threatening. The other factor is for reasons we don’t understand, our immunity to the common cold coronaviruses doesn’t seem to last very long, 6-months to a year. It’s not sure if a vaccine would work any better. Given enough time and research, we could probably make one, but people have decided it’s probably not worth the effort, again for something that’s not that bad of a disease.
There is a real concern that might also be true for this coronavirus. It’s possible that a vaccine to SARS-Cov-2 will only protect you for a 6-12months, which means you’ll need to be revaccinated every year, or even multiple times a year to keep up immunity. However, in this case, this virus causes enough of a disease, and affects enough people, that a vaccine would still be worth the effort.
Ms. Stremic: Does increasing temperature denature the proteins on the surface of the virus to destroy its shape? (based on videos circulating the internet claiming hairdryers and saunas can destroy it)
Dr. Matt Koci: So yes heating viruses, hot enough, long enough, will denature their proteins in ways that inactivate them. How hot and how long varies with different viruses, and it depends on what the virus is in. If it’s in water, it tends to be more susceptible to heat than–say–if it’s in snot. The extra proteins in snot help protect it. In many ways that’s what your body is trying to do when you get a fever. It’s trying to heat the place up (your body) but the fever is also a dangerous part of the disease. While you can sit in a sauna that is 140F, the cells of your body can’t handle that temperature. That’s why you sweat so much in a sauna to keep your core temp down. When your core body temp gets above 105F you are in serious danger.
To inactive viruses by heat you typically have to heat it up to 140-150F for several minutes (some viruses need even higher temps for longer). So yes, heat can destroy the virus, but you have to literally cook yourself to do it, so you’re dead anyway. A virology teacher I had years ago loved to say “viruses are the easiest pathogen to get rid of. If you want to kill the virus, kill the host.” But that doesn’t provide the medical outcome most people are hoping for, so the hairdryer and sauna are not going to help. If you’re still alive, so is the virus.
Check out Prof. Rob Dunn’s conversation with Dr. Matt Koci and other virus experts here.


